Syphilis
Outbreak Training Website
History of syphilis prior to the outbreak
Prior to the current outbreak, significant reductions in infectious syphilis had occurred among Aboriginal and Torres Strait Islander people living in remote areas with previously endemic (consistently high) levels of syphilis. Factors likely to have contributed to these reductions include the widespread use of antibiotics, effective syphilis screening programs and regionally-based syphilis registers that have assisted with improved case detection and appropriate management.1
Rates of gonorrhoea, chlamydia and trichomoniasis have been very high for many years, primarily reflecting a comparatively young age of the Australian Aboriginal and Torres Strait Islander population (mean age 23 years vs 38 years for entire population). Secondly, people living in regional, rural and remote areas can experience poorer health outcomes due to challenges in accessing healthcare, competing priorities, health messaging, lack of stable health workforce, employment, housing and other social and financial factors.
Overview of current outbreak
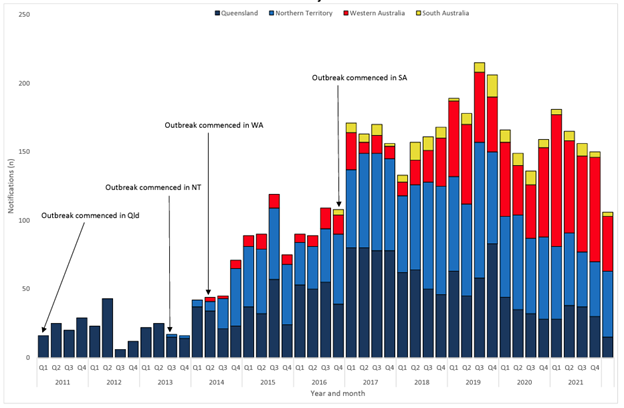
Graph: Notifications of category 1 (residing in declared outbreak region) infectious syphilis outbreak cases notified in Aboriginal and Torres Strait Isalnder people residing in affected retions of Queensland, the Northern Territory, Western Australia and South Australia from commencement of the outbreak in each juristiction to 31 March 2022: National Syphilis Surveillance Quarterly Report Quarter 1: 1 January - 31 March 2022
An outbreak of infectious syphilis among people living largely in remote and regional areas was first reported in northwest Queensland in January 2011. Over the years, the outbreak spread to other jurisdictions including the Northern Territory (NT), Western Australia (WA) and South Australia (SA).
References:
- 1Ward JS, Guy RJ et al. Epidemiology of syphilis in Australia: moving towards elimination of infectious syphilis from remote Aboriginal and Torres Strait Islander communities? Med J Aust 2011; 194 (10): 525–529.
- National update on HIV, viral hepatitis, and sexually transmissible infections in Australia: 2009–2018. Sydney: Kirby Institute, UNSW Sydney, https://kirby.unsw.edu.au/sites/default/files/kirby/report/National-update-on-HIV-viral-hepatitis-and-STIs-2009-2018.pdf
- National Syphilis Surveillance Quarterly Report Quarter 1: 1 January to 31 March 2021, https://www.health.gov.au/sites/default/files/documents/2022/06/national-syphilis-surveillance-quarterly-reports-2021.pdf
- The Kirby Institute. Tracking the Progress 2020: National Aboriginal and Torres Strait Islander BBV and STI Strategy. https://kirby.unsw.edu.au/sites/default/files/kirby/report/Tracking-the-progress-2020_National-ATSI-Strategy.pdf